More results...
More results...
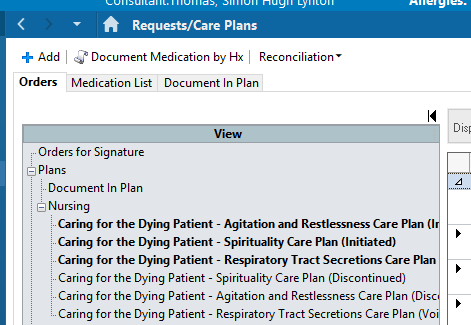
Open the Requests/Care Plans section of the Patient Record. This should show a list of all the patient’s Care Plans for this encounter.
At the top of the screen, you should have 3 tabs. When you open the page, it will normally direct you to the “Orders” tab, however to document on a Care Plan, we need to be on the “Document in Plan” tab.
When you enter the “Document in Plan” tab, you will be shown a list of all the patient’s active care plans. Inside the list, there will be a breakdown of all the initiated components in the plan. These are the parts we need to individually document.
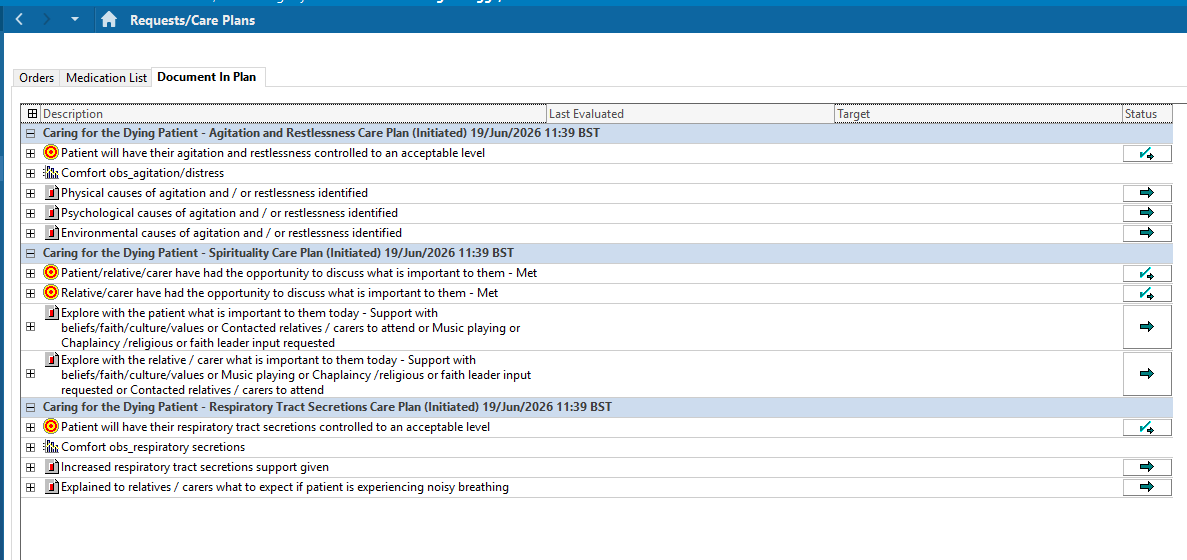
To document on a component, click on the component’s line. You should have a menu on the right-hand side of your page. This is where you can document the time of evaluation, whether the target/task was met or not met, reasons why it may not have been met and if any subsequent interventions have happened.
It is STRONGLY recommended that you add comments to your documentation in addition to the drop down menus. This gives the senior staff more information, helping them make better decisions for the patient’s interest and explain them to families or loved ones.
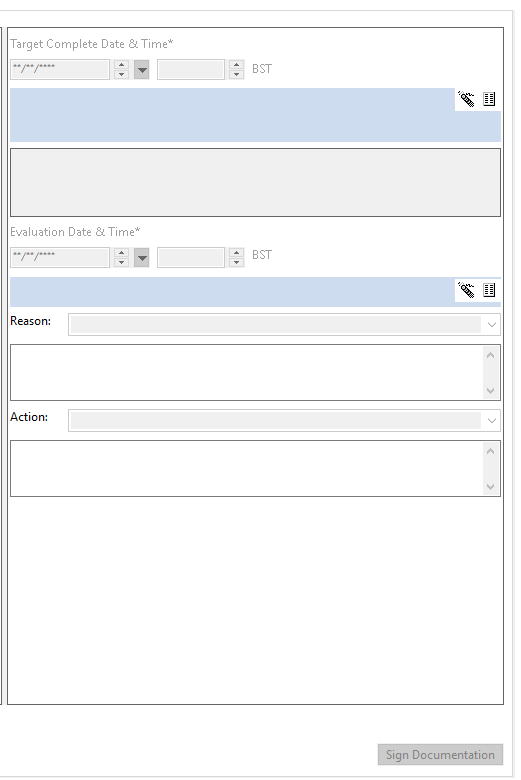
Once all the fields have been completed, you can click “Sign Documentation” in the bottom right corner. This will save all the lines you have documented on. You do not have to do this step for every component line you complete. On the Document in plan page, there will be ticks and crosses showing what has/has not been achieved for the patient.
